

Safe and Effective

COVID-19 breakthrough cases driving viral variants, new California study shows
One new study from California reveals some alarming news about the impact of these allegedly “rare” breakthrough cases. The study, based out of the University of California San Francisco (UCSF) and currently available online as a preprint, collected data from 1,373 people from hospital and community settings diagnosed with COVID-19 in the San Francisco area between February and June 2021. 9.1% of the sample (n = 125) were breakthrough COVID-19 infections, meaning they occurred in people who were fully vaxxed.
After analyzing genomic sequences and viral loads, the study authors came to several important conclusions.
First, fully jabbed people were more likely than unjabbed people to be infected by variants of SARS-CoV-2 that had decreased antibody neutralization (antibody neutralization is part of the immune system’s way of preventing viruses from getting into a cell). “These findings suggest that vaccine breakthrough cases are preferentially caused by circulating antibody-resistant SARS-CoV-2 variants,” explain the researchers.
In other words, fully jabbed people were more likely to be infected with antibody-resistant variants, which calls into question how “effective” these shots really are.
Second, vaccinated and unvaccinated people had equal levels of viral loads overall – meaning they had equal amounts of detectable virus in their bodies. This is important because the viral load is one way to measure how likely someone is to infect others; the higher the viral load, the more infectious a person is.
What this suggests is that being jabbed does not reduce the chances that someone will spread COVID-19 if they end up getting infected with SARS-CoV-2 – that is, if the shot doesn’t do what it’s supposed to do and protect a person from getting infected. Of course, the CDC no longer says that the shot is supposed to prevent infection – only that it is supposed to prevent severe illness, hospitalization, and death. Do you see how much they have moved the goalposts?
Third, COVID-19 positive people who show symptoms have higher viral loads compared to COVID-19 positive people without symptoms – and this was true whether they were jabbed or unjabbed. As the researchers put it, “symptomatic breakthrough infections may potentially transmit COVID-19 as efficiently as unvaccinated infections.”
In light of this data, it’s not surprising to hear that nearly a third of all July COVID-19 cases in Los Angeles occurred in people who were fully jabbed.
COVID-19 shots are supposedly “safe and effective” for preventing hospitalization and death, but not for preventing disease spread … so why the push for extra doses and injections in children?
Studies like this one from UCSF suggest that jab-resistant variants of COVID-19 are circulating, and jabbed people can catch and spread these variants, too – possibly more easily than unjabbed folks can. And the blame cannot be placed squarely on unjabbed people, since the COVID-19 shot cannot prevent infection, according to the CDC.
It’s a major logical inconsistency. Fully jabbed people can get COVID-19, and if they do, they can be just as likely to spread COVID-19 as people who don’t get the jab. So, why are fully jabbed people not being fired en masse, as well, nor being subject to weekly testing and public segregation?
Remember: taking the COVID-19 shot means you assume the full risk of the shot itself – and you STILL might get sick anyway. Is this risk-benefit ratio worth it for young, healthy people, including children, who are unlikely to get severely sick and far more likely to die of drowning than die of COVID-19?
Moderna and Johnson & Johnson are seeking authorization for booster shots this month, and Pfizer is seeking Emergency Use Authorization for 5-11-year-old kids.
How Many Have Died From the COVID Jabs?
According to Steve Kirsch, the COVID shots have already killed an estimated 200,000 Americans, a far higher number than the 15,386 deaths reported to the U.S. Vaccine Adverse Event Reporting System (VAERS) as of September 17, 2021. You can find all the research for Episode 1 of the “False Narrative Takedown” series on SKirsch.io/vaccine-resources.
Here is Steve Kirsch’s video on Rumble, click on this link
As noted by Kirsch, Centers for Disease Control and Prevention director Dr. Rochelle Walensky claims no causative link has been found for any of these deaths. She’s not lying, per se. But she’s also not telling the whole truth.
So far, the CDC has not determined that any death was directly caused by the COVID shot, but that doesn’t mean the injections haven’t killed anyone. In this episode, Kirsch sets out to determine whether evidence of causality exists, and if so, what the actual death toll is likely to be.

Alex Berenson reported that Iceland also has paused the Moderna shots.
Can VAERS Data Demonstrate Causality?
The big disconnect, Kirsch points out, is that the CDC insists that VAERS, as an early warning system, cannot prove (or disprove) causality. Kirsch argues that this is false. The idea that VAERS cannot show causality is part of how and why the CDC can claim none of the deaths is attributable to the COVID shot.
To prove his point, Kirsch gives the following analogy: Suppose you give a two-dose vaccine. After the first dose, nothing happens, but after the second dose, people die within 24 hours of a deep vein thrombosis (DVT). When you look at the VAERS data, what you would find is no reports associated with the first dose, and a rash of deaths after the second dose, and all within the same timeframe and with the same cause of death.
According to the CDC, you cannot ascribe any causality at all from that. To them, it’s just random chance that everyone died after the second dose, and from the same condition, and not the first dose or from another condition.
Kirsch argues that causality CAN be identified from this kind of data. It’s very difficult to come up with another explanation for why people die exactly 24 hours after their second dose.
For example, is it reasonable to assume that people with, say, undiagnosed heart conditions would die exactly 24 hours after getting a second dose of vaccine? Or that people with undiagnosed diabetes would die exactly 24 hours after their second dose?
Why not after the first dose, or two months after the second dose, or any other random number of hours or days, or for other random cause of death? Why would people randomly die of the same condition at the exact same time, over and over again?
Vaccine Program Needs To Be Halted Immediately
According to Kirsch, the vaccination program should be immediately halted, as the VAERS data suggest more than 200,000 Americans have already died, and more than 2 million have been seriously injured by the vaccines. Interestingly enough, Kirsch and his entire family took the COVID shot early on, so he’s not coming from an “anti-vax” position.
Ending the vaccinations would not spell disaster in terms of allowing COVID-19 to run rampant, as we now know there are safe and effective early treatment protocols that everyone can use, both at home and in the hospital. These treatments also work for all variants.
According to Kirsch, the CDC, the U.S. Food and Drug Administration and the National Institutes of Health are all “spreading misinformation about the vaccine versus early treatment.” In a nutshell, these agencies are saying the complete opposite of what is true — classic Orwellian doublespeak.
They claim the COVID shots are safe and effective, when the data show they’re neither, and they say there is no safe and effective early treatment, which is clearly false. At the same time, our medical freedoms are being stripped away under the guise of public health — all while an immense death toll is allowed to take place right before our eyes.
Kirsch is so confident in his analyses, he’s offered a $1 million academic grant to anyone who can show his analysis is flawed by a factor of four or more. So far, no one has stepped up to claim the prize. He’s even offered $1 million to any official willing to simply have a public debate with him about the data, and none has accepted the challenge.
As noted by Kirsch, “we’ve replaced debates as a way to settle scientific disagreements … with government-driven censorship and intimidation.” Medical recommendations are now also driven by the White House rather than medical experts and doctors themselves.
False Narratives Overview
Kirsch goes through five false narratives about COVID jab safety, namely that:
The shots are safe and effective
No one has died from the COVID shot
You cannot use VAERS to determine causality
The SARS-CoV-2 spike protein is harmless
Only a few adverse events are associated with the shots and they’re all “mild”
He also reviews the five false narratives about what the solutions are:
Vaccines are the only way to end the pandemic
Vaccine mandates are therefore needed
Masks work
Early treatments do not work
Ivermectin is dangerous
Merck and Pfizermectin


From Dr. Saladino:

Given the evidence available, it’s very hard to believe they AREN'T suppressing adjunctive treatments like Ivermectin in favor of profits.
And it’s not like shady stuff like this hasn’t happened before...
In 2009 Pfizer were fined $2.3 billion by the FDA for fraud…
And we’ve seen similar things with the tobacco industry…
And the sugar industry.
The mainstream media say Ivermectin is only a horse dewormer used by low IQ anti-science folks...
And Instagram, YouTube and Facebook are silencing anyone who talks about or even asks questions about it.
I can’t even say the word Ivermectin on Instagram for fear of my account being deleted again!
It’s a freaking disgrace that profits seem to be taking precedence over people’s health.
I’m not interested in Ivermectin as an alternative to vaccination as much as what it reveals about big pharma’s attitudes towards profit vs health.
And I support everyone making their own choice with regards to vaccination.
I do see data showing that vaccines can reduce hospitalizations and the severity of disease...
But the vaccinated are still getting Covid:
This paper published September 30th shows the vaccines are not only failing to prevent case numbers, but they are actually finding a positive association between vaccination rates and case numbers…
And if you look at the UK data right now the vaccinated cases are outnumbering the unvaccinated cases in all age groups above 18.
The vaccines are clearly not stopping people from getting Covid…
So why can’t we at least consider Ivermectin as an adjunctive therapy?
Dr. Pierre Kory MD has testified in front of the US Senate that Ivermectin has a powerful role to play in the treatment of Covid…
And he co-authored this Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19…
But the mainstream media are still painting him and his colleagues as ‘fringe’ and ‘anti-vaxx’...
Ivermectin: Horse dewormer or lifesaving intervention for COVID-19, with Pierre Kory, MD
COVID Shot Kills Five Times More People Than It Saves
Kirsch cites information from Dr. Peter Schirmacher, chief pathologist at the University of Heidelberg, who is recognized as one of the top 100 pathologists in the world.
Schirmacher did autopsies on 40 patients who died within two weeks of their COVID jab, and found 30% to 40% of them were conclusively due to the shot, as there was no other underlying pathology that could have caused the deaths. Now, he did not rule out that 100% of the deaths could have been caused by the shots. He just could not conclusively prove it.
There’s also Pfizer’s six-month study, which included 44,000 people. During the blinded period of the study, the deaths were just about even — 15 deaths in the vaccine group and 14 in the control group. So, one life was saved by the shot.
But then, after the study was unblinded and controls were offered the vaccine, another three in the original vaccine group died along with two original placebo recipients who opted to get the shot. None of these deaths was considered related to the Pfizer “vaccine,” yet no one knows what they actually died from.
So, the final tally ended up being 20 deaths in the vaccine group and 14 deaths in the control group. What this tells us is the Pfizer shot offers no all-cause mortality benefit. The shot saved one life, and killed six, which gives us a net-negative mortality rate. The reality is that five times more people are killed by the shot than are saved by it.
How to Calculate Excess Mortality
Kirsch explains how anyone can calculate the number of COVID shot deaths using VAERS data. What we’re looking at here is excess deaths, not background deaths of people who were going to die from a natural cause, such as old age, anyway. In summary, this is done by:
Determining the propensity to report
Determining the number of domestic deaths in the VAERS database
Determining the underreporting factor for serious events
Determining the background death rate, i.e., all deaths reported to VAERS by year
Calculating the number of excess deaths
Lastly, you would validate your findings using independent methods or comparing it to what others have found. Step-by-step instructions and calculations can be found in the document called “Estimating the Number of Vaccine Deaths in America.”
More Than 200,000 Have Likely Been Killed by the Jabs
Between the documentation on his website and the video, you get a detailed in-depth understanding of how to do this and how Kirsch came to the conclusions made. Here, I will simply provide a summary rundown of Kirsch calculations and conclusions:
Propensity to report = same as in previous years
Number of domestic deaths in the VAERS database = 6,167 as of August 27, 2021
Under-reporting factor for serious events = 41 (i.e., for every 41 events, only one is reported)
Background VAERS death rate = 500 per year (this background death number will be subtracted twice, as most COVID jab recipients are receiving two doses. This gives us a very conservative estimate)
Excess deaths calculation = (6,167 – 2 x 500) x 41 = 212,000 excess deaths
Using the same calculation methods, Kirsch conservatively estimates more than 300,000 Americans have also been permanently disabled by the COVID shots. These estimates have been validated by four teams of researchers using other methods. (None of them used VAERS data.)
If you’re under the age of 50, your risk of dying from the vaccine is greater than your chance of dying from COVID-19.
Kirsch also demonstrates another calculation to show the COVID shots kill more people than the actual COVID-19 infection does. That calculation also shows that if you’re under the age of 50, your risk of dying from the vaccine is greater than your chance of dying from COVID-19, so it makes no sense from a risk-benefit perspective to get the jab if you’re younger than 50.
What’s more, since your risk of natural infection exponentially decreases over time (as natural herd immunity grows, your chance of infection approximately halves each year), the risks of the COVID shot rapidly outgrow any potential benefit with each passing year.
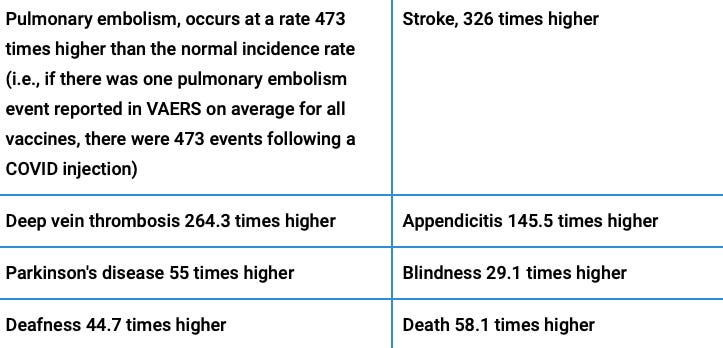
Examples of Adverse Events
Kirsch has also analyzed adverse events by symptom, calculating the rate at which they occur after the COVID shots compared to the average rate seen for all other vaccines combined from 2015- to 2019 for ages 20 to 60.
Interestingly, the most common cause of death in children aged 12 to 17 who got the COVID shot was pulmonary embolism. This was determined by the CDC’s Advisory Committee on Immunization Practices (ACIP) after analyzing the deaths of 14 children. Coincidence? Or evidence of causality?
Anecdotes and Other Data Consistent With High Death Rate
Kirsch also cites anecdotal data that can clue us into what’s happening. One top neurologist claims to have 2,000 reportable vaccine injuries in 2021, compared to zero in the last 11 years.
In all, 5% of her existing patients now have suspected vaccine injuries. Yet this neurologist has only reported two of them, because she got so frustrated with the VAERS system. So, in this instance, the under-reporting rate is not 41, but 1,000. And she’s not alone. This is another classic real-world illustration of what the PA Deborah Conrad, the VAERS Whistleblower shared with Del BigTree of the HighWire.
Canadian physician Dr. Charles Hoffe has also reported that 60% of his COVID jabbed patients have elevated D-dimer levels, which is indicative of blood clotting, and levels in many cases remained elevated for up to three months.
This too is evidence of causation, because your D-dimer level is a marker for blood clotting. Even if you don’t have obvious symptoms of clotting, it can indicate the presence of microclots. Hoffe discusses this in the video below.
Dr. Peter McCullough has also reported that troponin levels are elevated in many vaccinated patients. Troponin is a marker for heart damage, such as when you’re having a heart attack or myocarditis (heart inflammation). A level between 1 and 4 is indicative of an acute or recent heart attack. In case of a serious heart attack, troponin can remain elevated for five days.
In many patients who have received the COVID jab, the troponin level is between 35 and 50(!) and remains at that level for up to two months, which suggests massive damage is occurring to the heart. Yet this is what they’re routinely labeling as “mild” myocarditis. There’s absolutely nothing mild about this level of heart damage.
No Rate of Injury or Death Is Too Great
Unbelievably, there seems to be no ceiling above which the death and disability toll is deemed too great. Why aren’t the FDA and CDC concerned about safety when more than half a million side effect reports have been filed? How come nearly 16,000 reported deaths haven’t set off emergency alarms and in-depth investigations? Historically, 50 deaths have been the cutoff point at which a vaccine is pulled.
Considering the unprecedented risks of these shots, I urge you to review as much data as you can before you jump on the booster bandwagon. Based on everything I’ve seen, I believe the risk of side effects is likely going to exponentially increase with each dose.
If you need a refresher on the potential mechanisms of harm, download and read Stephanie Seneff’s excellent paper, “Worse Than The Disease: Reviewing Some Possible Unintended Consequences of mRNA Vaccines Against COVID-19,” published in the International Journal of Vaccine Theory, Practice and Research in collaboration with Dr. Greg Nigh.